
For most people their body weight is a personal issue. However people living in larger bodies face hurtful stigma including language surrounding obesity and overweight. Developed by Obesity Canada and the Canadian Association of Bariatric Physicians and Surgeons, the new Canadian Adult Obesity Clinical Practice Guidelines represent the first comprehensive update in Canadian obesity guidelines since 2007.[1]
Decades of research in behavioral and nutrition science suggest that it’s time to update our clinical approach and recognize that some patterns of communication about body weight are more helpful than others. Registered dietitians are deeply involved in this discussion and here are some of the topline messages from leading experts that stood out to us:
- Body Mass Index (BMI) is NOT an accurate tool for identifying obesity related complications [2]
BMI is a widely used tool for screening and classifying body weight but it’s been controversial for decades. A person’s BMI number is generated by considering their height in relation to their weight and it tells us about the size of the person’s body. Experts now agree that more information than BMI is needed to determine whether a person is sick or healthy. - Patient-centered, weight-inclusive care focuses on health outcomes rather than weight loss 1,2
Remember to ask permission before discussing body weight and respect the person’s answer. Health issues are measured by lab data and clinical signs. These can include blood pressure, blood sugar or reduced mobility. Shift the focus toward addressing impairments to health rather than weight loss alone. - Obesity is NOT simply a matter of self-control and the ‘eat less, move more’ advice is insufficient1
The effects of a dieting lifestyle are burdensome. Evidence-based advice must move beyond simplistic approaches of ‘eat less and move more’. For example, in recent years researchers gained a better understanding of clinical evidence and body weight biology. These include the amount of food energy absorbed through the gut, the brain’s role in appetite regulation and the thermic effect of eating.[3] Environmental factors such as where people live, work and food availably also have an influence on body weight. - People of higher weights should have access to evidence informed interventions, including medical nutrition therapy
There is a lot of misinformation about body weight so evidence-based health management is key. One of the recommended interventions is to include personalized counselling by a registered dietitian with a focus on healthy food choices and evidence-based nutrition therapy. - Recognize and address weight bias and stigma
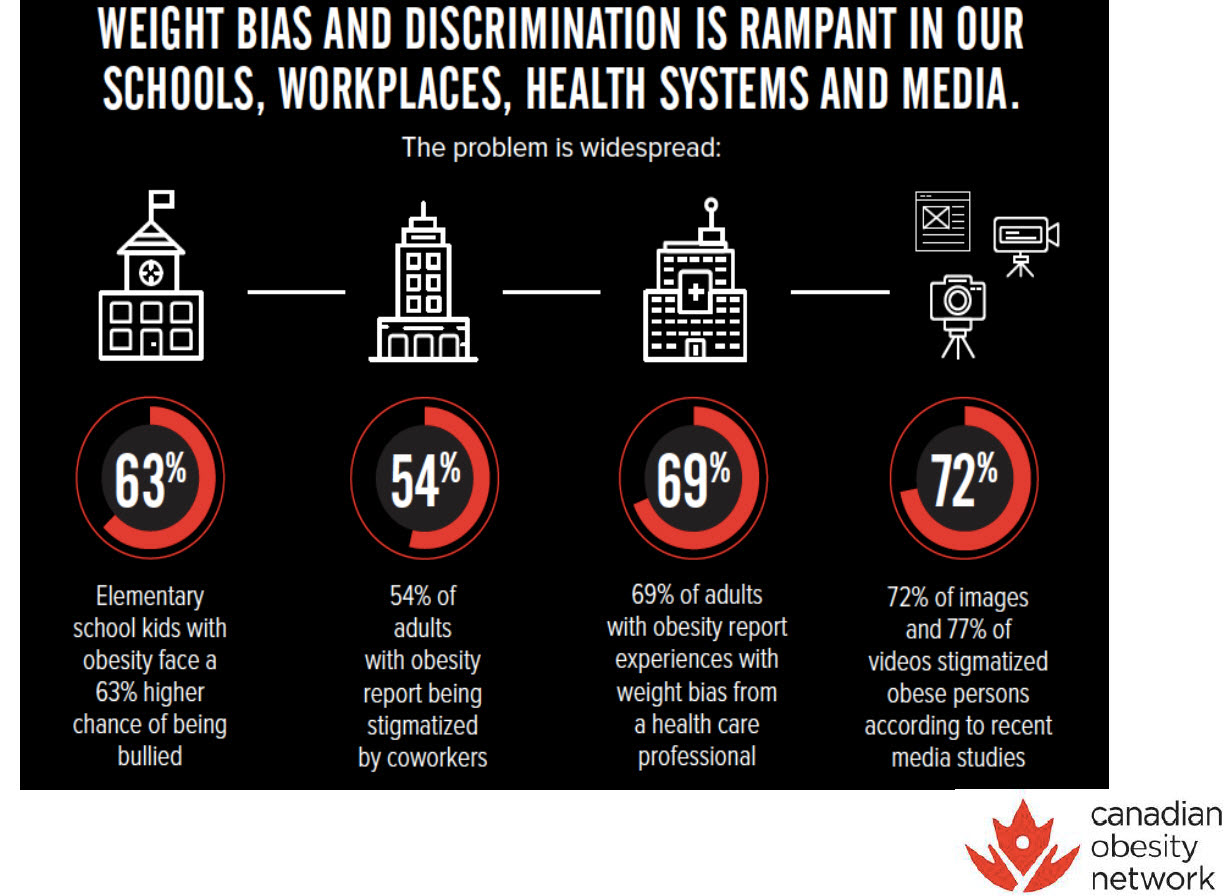
People with excess body weight experience weight bias and stigma. Weight bias is defined as negative weight–related attitudes, beliefs and judgements toward people who are of higher weight. This thinking can result in stigma which is acting on weight-based beliefs such as teasing, bullying, macroaggressions, social rejection and discrimination towards people living in larger bodies. People may also internalize weight stigma and criticize themselves or others based on body weight.
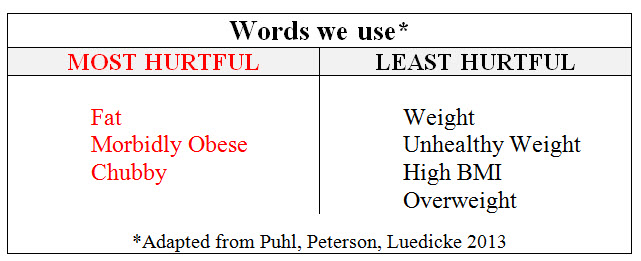
Experts consider that changes to language can alleviate the stigma of obesity within the health-care system and support improved outcomes for both people living in a larger body and for the health-care system. 3,[4],[5],[6]
In our Body Weight Words Matter! chart below we provide several examples of communication interventions to help assess your attitude and reduce body weight bias. Body Weight Words Matter INFOGRAPHIC N4N (Click here to download your copy of the PDF Body Weight Words Matter INFOGRAPHIC N4NN ) 
References:
[1] Obesity Canada (2020) Canadian Adult Obesity Clinical Practice Guidelines (CPGs) https://obesitycanada.ca/guidelines/
[2] Obesity Canada (2020) CMAJ Obesity in adults: a clinical practice guideline https://www.cmaj.ca/content/cmaj/192/31/E875.full.pdf
[3] Rubino et al. (2020) Joint international consensus statement for ending stigma of obesity. Nature Medicine www.nature.com/medicine
[4] Obesity UK (2020) Language Matters: Obesity https://cdn.easo.org/wp-content/uploads/2020/07/31073423/Obesity-Language-Matters-_FINAL.pdf
[5] Puhl, R. et.al (2016) Cross-national perspectives about weight-based bullying in youth: nature, extent and remedies. Pediatric Obesity,
[6] Puhl R., Peterson J. L., Luedicke J. (2013). Motivating or stigmatizing? Public perceptions of weight-related language used by health providers. Int. J. Obes. https://www.nature.com/articles/ijo2012110









 Dr. Ayra Sharma
Dr. Ayra Sharma Ted Kyle
Ted Kyle Sue Mah
Sue Mah